Brostrom Procedure - Ankle Ligament Surgery
HOME
In this article, we'll look briefly at a popular surgery used to repair ankles. It is known as "The Brostrom Repair" or "The Brostrom Procedure."
NEED FOR CORRECTIVE SURGERY: If an ankle becomes unstable to the point where a person can't function normally, surgery may be necessary to fix the problem. The common term for this weakness is chronic ankle instability, sometimes abbreviated as CAI. Anatomically, the ligaments become prolapsed, or infirm, and no longer hold the bones of the ankle joint together as efficiently. This can be surgically corrected.
CAUSES: CAI is caused by repeated sprains, especially sprains not properly taken care of, resulting in permanent ligament damage. Sprains can result in thinning, stretching, or partial/complete tearing of the ligaments. Some people may not have had repeated sprains but have had incidents where the ligaments have torn to the point where they cannot heal on their own. Usually a patient has had multiple sprain events over a period of years before surgery is necessary to retain the integrity of the ankle joint. Less often, a patient may have a congenital disorder where the ligaments are anatomically weaker. CAI is often first discovered during childhood, if the child is frequently experiencing ankle sprains, especially if they are active in sports. Sometimes this can continue into adulthood.
Doctors will usually try some more conservative treatments before suggesting ankle surgery. They include physical therapy, cortisone or other shots, and various bracing (boot or cast or ankle brace) if the patient has an acute injury. As you can probably imagine, these things usually provide only temporary relief, as the underlying problem with the compromised ligaments has not been resolved. If the ankle problems become unbearable and unmanageable, surgery is the final stop on what for most CAI patients is a long road.
SYMPTOMS: The ankle feels weak, as if it will collapse or not support the foot anymore. This can occur in one or both ankles but most patients experience significantly more problems with one ankle or the other. Pain and swelling are almost always present upon more aggressive physical activity but they can also occur while at rest. The ankle will frequently sprain. Many patients with CAI have the characteristic symptom of a loud clicking or grinding noise upon plantar (toes pointed down) and dorsal flexion (toes pointed up.) This sound is characteristic of hypermobility and usually indicates that the patient has lost full functionality of the ankle.
This instability is characterized by a marked propensity of the ankle to roll inward (the foot slips out from under the ankle joint, so to speak), leading to frequent spraining, and further weakening the ligaments.
Sometimes the ligamentous laxity and frequent spraining are a consequence of anatomical shape of the foot. Those who have very high foot arches and/or foot supination, often have weak ankles that will give out, and sprain, easily. The mal-formed foot often looks like it has an inward tilt instead of sitting more or less "flat on the ground." If this is the case, doing a ligament repair surgery may only have short-term effectiveness in the long term because the underlying
anatomical problem has not been resolved. Foot reconstruction surgeries can be complicated and often have a very long recovery period.
Here is a video I made after my own Brostrom surgery. If you don't want to read the rest of this article, watch the video!
"The Brostrom" Procedure:
Most repairs done to the ATF and CFL ligaments of the ankle are done by what is known as the Brostrom Procedure. Sometime in the 1960s, an orthopedic surgeon named Brostrom developed a procedure for anatomical repair in response to many patients having CAI. Since that time, it has undergone some revisions and modifications by various surgeons, and today a 'modified Brostrom Procedure' is usually done on the patient. It is sometimes also known as the Brostrom-Gould Procedure.
The Brostrom surgery is often not recommended for patients who do competitive sports because the state of the ankle may return to the compromised pre-surgical state. Patients who formerly did competitive sports are often urged to reduce their activity levels post-surgically and only engage in them with appropriate bracing of the ankle joint.
The diagnosis of a compromised ankle may or may not be made with x-rays or MRI scans. An experienced podiatrist can usually assess 90% or more of the situation just from a physical exam and discussion with the patient as to their
day-to-day symptoms. The x-rays are of very limited use, and although an MRI scan will show significant ligament and tendon injury, especially if it was recent, it will usually not elucidate ligament issues such as hyperlaxity. If the decision to operate is agreed upon by doctor and patient, the surgery will be scheduled.
THE SURGERY:
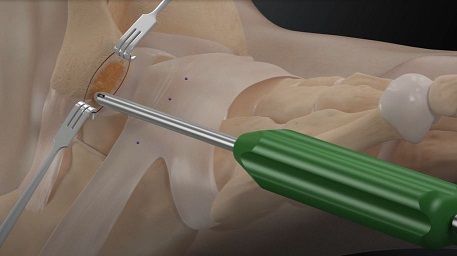
1. The Brostrom Procedure is done in a surgery center or hospital operating facility. It is not done in an orthopedic medical office because a sterile environment is required. The patient is admitted into the facility and undergoes general anesthesia for the procedure (less often, a patient may instead be given a nerve block and given conscious sedation). The procedure usually takes between 1 and 2 hours depending on the state of the ligaments. The surgeon will tighten the ATF and CFL ligaments surgically. The damaged tissue will be removed and small holes will be drilled into the fibula (smaller bone of the leg) through which sutures are placed. If the damage to the ligaments is significant, cadaver ligamentous material may be inserted. This is actually a fairly simple repair procedure.
2. Details as to the surgery can found here, in this excellent Youtube video.
3. Once the repair is finished, a short leg plaster splint or cast is applied so the ankle is completely locked. The patient usually goes home the same day of the surgery. The patient will be non-weight bearing, on crutches for 6 weeks*. The patient will usually take painkillers for 2 weeks. *Some doctors will require less time, but much less than 6 weeks is not advisable.
4. The patient visits the orthopedic doctor's office the week following surgery. The splint or cast is opened just enough to check the healing of the incision, then re-applied. The patient returns
a week or two later and the incision sutures are removed. If the patient is in a splint, it is usually removed at this point and replaced with a hard cast that remains on for another 3-4 weeks. The patient usually remains on crutches until this cast comes off. Patients are generally advised not to travel a long distance away, especially by air, until the wound sutures are out and a second splint or cast is on. N.B. the surgical sutures in the ankle remain there permanently! These are never removed!
5. At approximately week 6 following surgery, the patient returns to the doctor's office for cast removal, at which point they are placed in either a walking cast (vastly preferable) or a pneumatic walking boot (aka ski boot-style 'CAM walker' - CAM is Controlled Ankle Movement). Crutch use is usually discontinued
at this point although some patients will often continue using them for another week or so if they experience pain upon walking again. This boot or second cast is worn for
another few weeks.
6. At approximately 9 weeks, the immobilization phase is complete and the patient can begin the second and longest phase of recovery as they slowly get back to normal activity. An AFO (ankle/foot orthotic) brace - a rigid but comfortable ankle brace that can be worn with a regular shoe - is worn every day for several more months to prevent rolling of the ankle. Physical therapy is not generally recommended because the ligaments need to stay firm and tight. The patient can simply do self-treatment of ice packs when the ankle and foot swell. This periodic swelling is normal and will gradually decrease over the months ahead.
7. At 16-20 weeks, the patient can slowly ease back into more aggressive physical activity, but always while wearing the brace to prevent disruption of the ankle repairs. Generally, recovery is nearly complete in the 6-8 month range depending on the patient, although it can be up to a year in some patients.
WHEN TO SEE A DOCTOR: If you have a history of repeated ankle sprains that become uncontrollable, along with symptoms that linger
long after a sprain episode, an appointment with a foot/ankle specialist should be made. Or if you simply have a dysfunctional, constantly painful ankle that feels like it's no longer supporting your foot when you walk, likewise, see a specialist. Doing a surgery like the Brostrom Procedure will not usually be the first line of treatment, but if a patient has all the hallmark symptoms of CAI, it will probably be suggested.
WHAT KIND OF DOCTOR TO SEE: You will need to see a podiatrist who specializes
in foot and ankle surgery. Some podiatrists do not do ankle surgery, or not as often. You need to select a doctor who has done ankle ligament repair surgery regularly for a long period of time and knows how to treat you from start to finish. These are usually sports medicine foot and ankle specialists. An experienced specialist knows exactly what is happening inside your ankle for the duration of your treatment and can devise a treatment plan for you very quickly, having done it on enough patients.
Again, it is NOT advisable to consult a general podiatrist who only works on simpler foot problems or who mainly focuses on minor surgeries/elective surgeries. They will usually not be able to give you the kind of treatment you need to maintain the integrity of your ankle.
If you have questions, please email me at info@castandcrutches.com I've had this surgery myself so am well prepared to advise!
References:
Arthrex, Inc.
Foot and Ankle Anatomy, by L. Lyons and I. Higgins. © 2000, Wolters-Kluwer Publishing.
Topics:
sprained ankle, broken ankle, knee injury, broken leg, dislocated ankle, sports injury, broken foot, crutches, sprained foot, stress fracture, ankle surgery, foot surgery, Brostrom procedure, modified Brostrom procedure, ankle injury, sprain, contusion, Achilles tendon, Achilles tendon rupture, plantar fasciitis, foot pronation, foot supination, traveling injured, handicapped, cast and crutches, camwalker, removable cast, leg cast
Go back to Main Page